
Tenodermodesis for the Treatment of Late-Presenting Tendinous Mallet Finger Deformities in Children and Adolescents
Article Sidebar
Main Article Content
Abstract
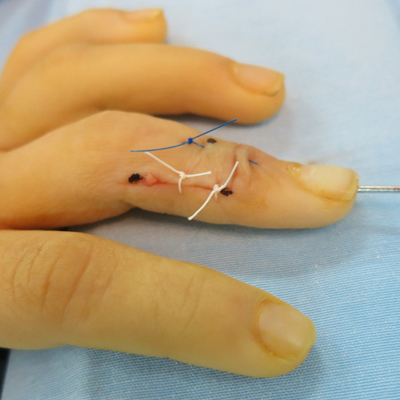
Materials and Methods: Nine patients (8 males) with an average age of 8.6±6 years (1-15 range) were retrospectively evaluated. The injury manifested at an average of 27±11.4 days after trauma (15-45 range). In 4 patients the mechanism was a laceration and, in 5, indirect trauma. Patients were treated by tenodermodesis and transitory fixation of the distal interphalangeal joint with a Kirschner wire. The average follow-up was 61±34.7 months (12-106 range). Active and passive range of motion of the distal interphalangeal joint (DIPJ), pain, deformity, limitations in everyday life activities, and need for further treatment were evaluated. Crawford criteria was used to evaluate the outcomes.
Results: The results were excellent in eight patients, and fair in one according to the Crawford criteria. One case required reintervention for re-rupture in a poorly collaborating patient. Two cases presented granuloma as a complication and required resection. No patients presented pain at the last follow-up, nor limitations in everyday life activities. Eight patients had full active DIPJ extension, and one had a 20° residual deformity.
Conclusion: Tenodermodesis allows anatomical reconstruction of the extensor mechanism in pediatric patients. The clinical results are encouraging in late-presenting lesions.
Level of Evidence: IV
Downloads
Metrics
Article Details
Manuscript acceptance by the Journal implies the simultaneous non-submission to any other journal or publishing house. The RAAOT is under the Licencia Creative Commnos Atribución-NoComercial-Compartir Obras Derivadas Igual 4.0 Internacional (CC-BY-NC.SA 4.0) (http://creativecommons.org/licences/by-nc-sa/4.0/deed.es). Articles can be shared, copied, distributed, modified, altered, transformed into a derivative work, executed and publicly communicated, provided a) the authors and the original publication (Journal, Publisher and URL) are mentioned, b) they are not used for commercial purposes, c) the same terms of the license are maintained.
In the event that the manuscript is approved for its next publication, the authors retain the copyright and will assign to the journal the rights of publication, edition, reproduction, distribution, exhibition and communication at a national and international level in the different databases. data, repositories and portals.
It is hereby stated that the mentioned manuscript has not been published and that it is not being printed in any other national or foreign journal.
The authors hereby accept the necessary modifications, suggested by the reviewers, in order to adapt the manuscript to the style and publication rules of this Journal.
References
https://doi.org/10.1007/s11552-014-9609-y
2. Bendre AA, Hartigan BJ, Kalainov DM. Mallet finger. J Am Acad Orthop Surg 2005;13(5):336-44.
https://doi.org/10.5435/00124635-200509000-00007
3. Valdes K, Naughton N, Algar L. Conservative treatment of mallet finger - A systematic review. J Hand Ther
2015;28(3):237-45. https://doi.org/10.1016/j.jht.2015.03.001
4. Kardestuncer T, Bae DS, Waters PM. The results of tenodermodesis for severe chronic mallet finger deformity in children. J Pediatr Orthop 2008;28(1):81-5. https://doi.org/10.1097/BPO.0b0131815ff31e
5. Shin EK, Bae DS. Tenodermodesis for chronic mallet finger deformities in children. Tech Hand Up Extrem Surg
2007;11(4):262-5. https://doi.org/10.1097/BTH.0b013e31812f5714
6. Sorene ED, Goodwin DR. Tenodermodesis for established mallet finger deformity. Scand J Plast Reconstr Surg
Hand Surg 2004;38(1):43-5. https://doi.org/10.1080/02844310310009528
7. De Boeck H, Jaeken R. Treatment of chronic mallet finger deformity in children by tenodermodesis. J Pediatr
Orthop 1992;12(3):351-4. https://doi.org/10.1097/01241398-199205000-00013
8. Waters PM, Benson LS. Dislocation of the distal phalanx epiphysis in toddlers. J Hand Surg Am 1993;18(4):581-5. https://doi.org/10.1016/0363-5023(93)90293-C
9. Iselin F, Levame J, Godoy J. A simplified technique for treating mallet fingers: tenodermodesis. J Hand Surg Am
1977;2(2):118-21. https://doi.org/10.1016/s0363-5023(77)80095-6
10. Garberman SF, Diao E, Peimer CA. Mallet finger: Results of early versus delayed closed treatment. J Hand Surg Am 1994;19:850-2. https://doi.org/10.1016/0363-5023(94)90200-3
11. Altan E, Alp NB, Baser R, Yalçın L. Soft-tissue mallet injuries: a comparison of early and delayed treatment. J Hand Surg Am 2014;39(10):1982-5. https://doi.org/10.1016/j.jhsa.2014.06.140
12. Auchincloss JM. Mallet-finger injuries: a prospective, controlled trial of internal and external splintage. Hand
1982;14(2):168-73. https://doi.org/10.1016/s0072-968x(82)80011-9
13. Bellemere P. Treatment of chronic extensor tendons lesions of the fingers. Chir Main 2015;34(4):155-81.
https://doi.org/10.1016/j.main.2015.05.001
14. Makhlouf VM, Deek NA. Surgical treatment of chronic mallet finger. Ann Plast Surg 2011;66(6):670-2.
https://doi.org/10.1097/SAP.0b013e3181e6d017
15. Ulkür E, Cengiz A, Ozge E, Celiköz B. Repair of chronic mallet finger deformity using Miteck micro arc bone
anchor. Ann Plast Surg 2005;5:393-6. https://doi.org/10.1097/01.sap.0000151464.03967.a2
16. Warren RA, Kay NR, Ferguson DG. Mallet finger: comparison between operative and conservative management in those cases failing to be cured by splintage. J Hand Surg Br 1988;13(2):159-60.
https://doi.org/10.1016/0266-7681(88)90127-1
17. Kon M, Bloem JJAM. Treatment of mallet fingers by tenodermodesis. Hand 1982;14(2):174-5.
https://doi.org/10.1016/s0072-968x(82)80012-0
18. Nakamura K, Nanjyo B. Reassessment of surgery for mallet finger. Plast Reconstr Surg 1994;93:141-149. PMID: 8278469
19. Doyle JR. Extensor tendons—acute injuries. En: Green DP, Hotchkiss RN, Pederson WC (eds). Green’s operative hand surgery, 4th ed. New York, NY: Churchill Livingstone; 1999:1962-87.
20. Crawford FP. The molded polythene splint for mallet finger deformities. Hand Am 1984;2(9):231-7.
https://doi.org/10.1016/s0363-5023(84)80148-3
21. Georgescu AV, Capota IMV, Matei IRG. A new surgical treatment for mallet finger deformity- Deepithelialised
pedicled skin flap technique. Injury 2013;44:351-5. https://doi.org/10.1016/j.injury.2013.01.013
22. Brzezienski MA, Schneider LH. Extensor tendon injuries at the distal interphalangeal joint. Hand Clin 1995;11:373-86. PMID: 7559816
23. Houpt P, Dijkstra R, Storm van Leeuwen JB. Fowler’s tenotomy for mallet deformity. J Hand Surg Br 1993;18:499-500. https://doi.org/10.1016/0266-7681(93)90157-b
24. Thompson JS, Littler JW, Upton J. The spiral oblique retinacular ligament (SORL). J Hand Surg Am 1978;3:482-7.
https://doi.org/10.1016/s0363-5023(78)80144-0
25. Kleinman WB, Petersen DP. Oblique retinacular ligament reconstruction for chronic mallet finger deformity. J Hand Surg Am 1984;9:399-404. https://doi.org/10.1016/s0363-5023(84)80231-2
26. Katzman SS, Gibeault JD, Dickson K, Thompson JD. Use of a Herbert screw for interphalangeal joint arthrodesis. Clin Orthop 1993;296:127-32. PMID: 8222414