Tendon Injuries of the Knee Extensor Mechanism: Treatment and Rehabilitation Protocol
Abstract
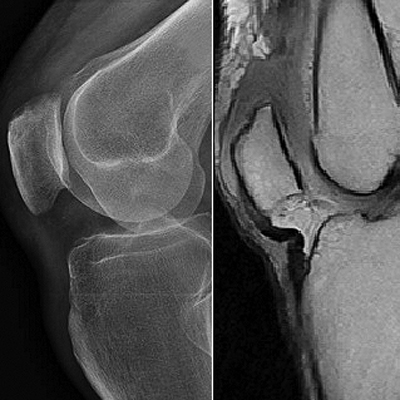
Background: The rupture of the extensor mechanism can have its origin at bone or tendon level. Its main cause is patellar fracture, followed by quadriceps tendon rupture, and, finally, patellar tendon rupture. These ruptures can be due to direct or indirect trauma. Tendon ruptures of the extensor mechanism are rare, developing with trauma related to the daily routine, sports, or associated systemic diseases. They represent 3% of all tendon injuries. Materials and Methods: We presented 22 tendon ruptures of the knee extensor mechanism, surgically treated between June 2015 and January 2019, from which eight (8) ruptures were of the quadriceps tendon (2 bilateral) and fourteen (14) of the patellar tendon (1 bilateral). The cases were evaluated using the Lysholm score, radiographs, and MRI. Results: The minimum follow-up was one (1) year. According to the results of those twenty-two (22) surgeries, thirteen (13) cases had excellent results, seven (7) cases were good and two (2) of them were fair. Conclusion: In cases of patellar tendon injury, the primary repair with transosseous suture plus figure-of-eight cerclage as augmentation provides a stable reconstruction, allowing the implementation of an early mobilization post-surgery protocol, thus achieving excellent functional outcomes with low complication levels.Downloads
References
Siwek CW, Rao JP. Ruptures of the extensor mechanism of the knee joint. J Bone Joint Surg Am 1981;63(6):932-7. PMID: 6985557
Blazina ME, Kerlan RK, Jobe FW, Carter VS, Carlson GJ. Jumper’s knee. Orthop Clin North Am 1973;4(3):665-78.
PMID: 4783891
Larson RV, Simonian PT. Semitendinosus augmentation of acute patellar tendon repair with immediate
mobilization. Am J Sports Med 1995;23(1):82-6. https://doi.org/10.1177/036354659502300114
Sivananthan S, Sherry E, Warnke P, Miller MD. Mercer´s textbook of orthopedics and trauma, 10th ed. London: CRC Press; 2012:368-497.
Meyer Z, Ricci WM. Knee Extensor mechanism repairs: standard suture repair and novel augmentation technique. J Orthop Trauma 2016;30(Suppl 2):S30-S31. https://doi.org/10.1097/BOT.0000000000000604
Rasul AT Jr., Fischer DA. Primary repair for quadriceps tendon ruptures. Results of treatment. Clin Orthop Relat
Res 1993; (289):205-7. PMID: 8472417
Scuderi GR, Easley ME. Quadriceps and patellar tendon disruptions. En: Insall JN, Scott WN (eds.). Surgery of the knee. New York: Churchil Livingstone; 2001:1074-86.
Tegner Y, Lysholm J. Rating systems in the evaluation of knee ligament injuries. Clin Orthop Relat Res
;(198):43-9. PMID: 4028566
Matas A. Diseño del formato de escalas tipo Likert: un estado de la cuestión. REDIE 2018;20(1):38-47.
Ilan DI, Tejwani N, Keschner M, Leibman M. Quadriceps tendon rupture. J Am Acad Orthop Surg 2003;11(3):192-200. https://doi.org/10.5435/00124635-200305000-00006
Shah MK. Simultaneous bilateral rupture of quadriceps tendons: analysis of risk factors and associations. South Med J 2002;95(8):860-6. PMID: 12190222
Rose PS, Frassica FJ. Atraumatic bilateral patellar tendon rupture. A case report and review of the literature. J Bone Joint Surg Am 2001;83(9):1382-6. PMID: 11568202
Costa Paz M, Makino A, Paniego G, Narváez R, Ayerza M, Muscolo L. Reparación quirúrgica mediante
tenodesis con anclajes óseos de los tendones del aparato extensor de la rodilla. Rev Asoc Argent Ortop Traumatol 2007;72(1):70-4. Disponible en: https://www.aaot.org.ar/revista/2007/n1_vol72/art12.pdf
Maniscalco P, Bertone C, Rivera F, Bocchi L. A new method of repair for quadriceps tendon ruptures. A case
report. Panminerva Med 2000;42(3):223-5. PMID: 11218630
Schliemann B, Grüneweller N, Yao D, Kösters C, Lenschow S, Roßlenbroich SB, et al. A biomechanical evaluation of different surgical techniques for treating patellar tendon ruptures. Int Orthop 2016;40(8):1717-23. https://doi.org/10.1007/s00264-015-3003-4
Bhargava SP, Hynes MC, Dowell JK. Traumatic patella tendon rupture: early mobilisation following surgical repair. Injury 2004;35(1):76-9. https://doi.org/10.1016/s0020-1383(03)00069-x
Manuscript acceptance by the Journal implies the simultaneous non-submission to any other journal or publishing house. The RAAOT is under the Licencia Creative Commnos Atribución-NoComercial-Compartir Obras Derivadas Igual 4.0 Internacional (CC-BY-NC.SA 4.0) (http://creativecommons.org/licences/by-nc-sa/4.0/deed.es). Articles can be shared, copied, distributed, modified, altered, transformed into a derivative work, executed and publicly communicated, provided a) the authors and the original publication (Journal, Publisher and URL) are mentioned, b) they are not used for commercial purposes, c) the same terms of the license are maintained.
In the event that the manuscript is approved for its next publication, the authors retain the copyright and will assign to the journal the rights of publication, edition, reproduction, distribution, exhibition and communication at a national and international level in the different databases. data, repositories and portals.
It is hereby stated that the mentioned manuscript has not been published and that it is not being printed in any other national or foreign journal.
The authors hereby accept the necessary modifications, suggested by the reviewers, in order to adapt the manuscript to the style and publication rules of this Journal.